Propranolol For Infantile Hemangiomas
Infantile hemangiomas (IHs) are benign tumors of endothelial cells that show a rapid proliferating phase usually followed by variable degrees of spontaneous regression.
Because of this unique behavior, most His can be left untreated, but His located in areas of particular concern, such as periorbital, oropharyngeal, preauricular, or parotid regions, may need rapid and active treatment to prevent permanent sequelae.
Corticosteroids have been considered the first-line therapy for severe or complicated IHs .
Other choices, including interferon-a, vincristine, laser therapy, topical imiquimod or surgical excision have been reported to be effective alternatives.
However, all these options have potential toward side effects or unknown long-term safety.
Recent reports of successful treatment of a small number of patients with the betablocker agent propranolol for IHs have led to considerable excitement and have prompted the large-scale use of propranolol for infants.
We present a multicenter open study describing the efficacy of propranolol in 71 children with IH and the adverse effects related to this therapy.
MATERIALS AND METHODS
Inclusion and Exclusion Criteria
Seventy-one patients from four different hospitals in Spain and Argentina were treated with oral propranolol for IHs between May 2008 and June 2009.
We included in our study cases of children younger than 4 years old with IHs that were considered to require treatment
because of one of the following reasons:
eyelid involvement with ocular risk of occlusion or compression;
airway obstruction; or large IHs with considerable aesthetic derangement or ulceration.
Patients previously treated with corticosteroids or surgery were also considered candidates for inclusion if prior modalities had failed.
Exclusion criteria included PHACES (Posterior fossa malformations, Hemangioma, Arterial anomalies, Cardiac defects, Eye abnormalities, Sternal clefts) syndrome, history of cardiac abnormalities, history of hypoglycemia, and history of asthma or bronchospasm.
While the study focused on infants, patients over 1 year of age were enrolled if IHs showed signs of continued
proliferation or did not show any signs of resolution since infancy
Evaluations Before and During Treatment
Before treatment, all patients underwent a cardiologic examination including clinical examination, electrocardiogram(EKG),and blood pressure measurements.
Monitoring of blood pressure and heart rate one to three times a day was performed during the first 2 or 3 days of treatment;
Further monitoring during the study included a cardiologic reevaluation at 1 to 4 weeks including physical examination and EKG , blood pressure, and heart rate measurements.
Monthly follow-up visits were scheduled for severity scoring of the IH, physical examination including blood pressure and heart rate, and adverse effect record, until the end of the treatment.
A cerebral magnetic resonance imaging/magnetic resonance angiography (MRI/MRA) and cardiac ultrasound were carried out in patients with segmental facial IHs before initiating therapy to rule out PHACES syndrome.
Dosage and Duration
All patients were treated with oral propranolol, 1 mg ⁄ kg ⁄ 12 hours, and this dosage was maintained during the whole period of study.
A treatment period of at least 12 weeks was scheduled, which could be further expanded if the patient required more time to achieve the resolution of the problem that had led to initiate propranolol therapy.
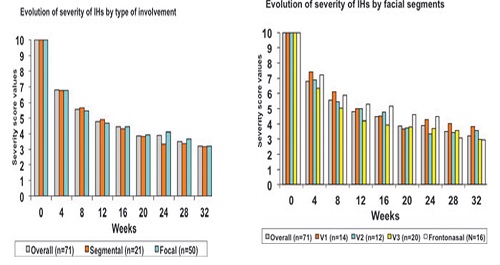
The response of infantile hemangiomas to propranolol was similar regardless of sex, age at onset of treatment, type of involvement (segmental and nonsegmental), facial segments affected, special locations (eyelid, nasal tip, and parotid region), ulceration, and depth of infantile hemangiomas.
Severity Scoring System
To measure the effect of the treatment, a photographbased visual scale was used.
Front and lateral pictures of every patient were taken before treatment and at everyfollow-up visit.
. Five of the investigators scored the severity of the IHs from 10 to 0, considering 10 as the original IH before treatment and 0 as completely normal skin.
A value of 5 indicated an estimated 50% reduction of the IH.
Size and color were the main features taken into account for the severity score of all IHs.
RESULTS
General Data
Seventy-one patients (15 male and 56 female, age range (1–45 mos) entered the study .
Fifty patients started therapy before 6 months of age, and in 21 patients the treatment was begun after 6months (mean age 5.8 mos, range 1–45 mos).
Five patients had subglottic IHs causing significant airway obstruction.
Propranolol had been the only treatment administered to 63 patients, Whereas four patients had been previously treated with corticosteroids and four with surgery.
In both instances, such treatments had failed to achieve significant improvement.
General Efficacy of Propranolol
By the time this paper was written, all patients but one had completed at least 12 weeks of treatment .
One infant failed to complete the 12-week period of study because of lack of efficacy, but his scoring values were included to avoid selection bias.
The longest treatment period was 44 weeks.
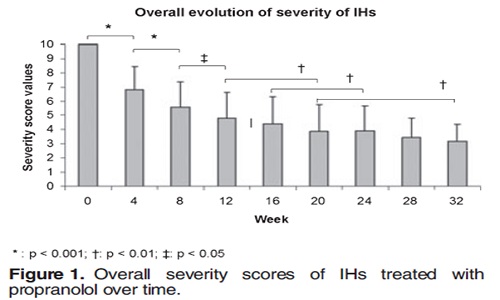
Overall, propranolol was a rapid and effective treatment for IHs in this series of patients .
At 4 weeks of treatment, the average score was 6.8 (p < 0.001 compared to the initial value).
At 8 weeks of treatment, the average score was 5.6
(p < 0.001 compared to the4 wks value);
at 12 weeks, the average score was 4.8.
at 16 weeks it was 4.4
At 20 weeks it was 3.9; at 24 weeks it was 3.9; at 28 weeks it was 3.5 and at 32 weeks it was 3.2 .
At 20 weeks of treatment, a mean score of 4 was achieved,thus indicating an average reduction of 60%.
Eight of 71 (11%) IHs had experienced a reduction of at least 50% in the severity score at 4 weeks, 24 of 71 (34%) at 8 weeks, and 42 of 71 (59%) at 16 weeks.
We observed that the reduction of the IH was more marked during the first 10 weeks of treatment, and the effect of propranolol on IHs seems to stabilize after week 20.
The mean duration of treatments was 20.0 weeks, and only 15 patients continued treatment for more than 32 weeks, achieving some further lesion reduction
Efficacy of Propranolol Within Different
Groups of Patients
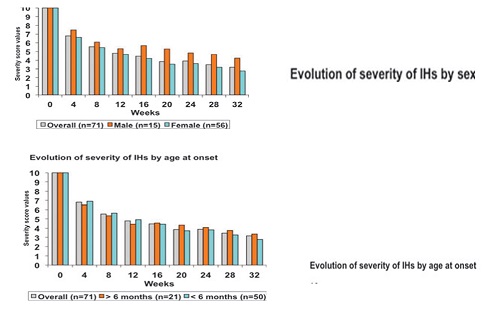
Efficacy was not influenced by gender, both male and female infants showed a similar reduction in severity scores throughout the study .
Propranolol therapy had similar effectiveness regardless of the age at
onset of treatment (before or after 6mos of age), indicating that IHs beyond the proliferating stage or late proliferating IHs seemed to respond to treatment.
Infantile hemangiomas affecting
the upper eyelid, the nasal tip, and the parotid region are often troublesome;
the reduction in the average severity score in these latter locations was very similar to the average reduction in the whole group, indicating that IHs of the
eyelid and parotid region also respond effectively to propranolol treatment.
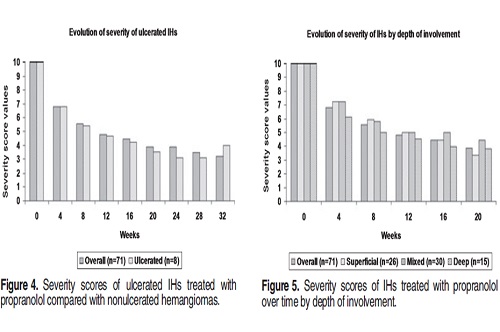
In eight patients, the IH was ulcerated;
the ulcerated IHs experienced a reduction in severity scorings similar to nonulcerated hemangiomas, and ulceration was completely resolved in all patients within 2 weeks of treatment .
Likewise, propranolol was equally effective for superficial, mixed, and deep IHs .
Five infants with extensive cutaneous hemangioma also had airway IHs causing air flow obstruction;
in all these children , air way obstruction dramatically improved, and they were free of dyspnea and stridor within a few days after starting propranolol therapy.
A few side effects were observed.
All patients had regular blood pressure monitoring; no patient showed symptomatic hypotension.
.
Hypoglycemia was not seen in 10 patients specifically tested.
Ten of 71 patients were noted to have agitated
sleep, and one had to discontinue the treatment after 3 weeks of propranolol because of this.
One patient suffered cyanotic breath-holding spells, which were still present after propranolol withdrawal.
One patient showed stridor not associated with airway IH, which lead to treatment withdrawal.
DISCUSSION
Propranolol is a nonselective b-blocker that blocks the action of adrenaline on both b1- and b2-adrenergic receptors.
Leaute-Labreze et al reported the effectiveness of propranolol for the treatment of IHs for the first time.
They presented the cases of 11 children with severe IHs, which improved after the first day of treatment.
Our series of patients confirms that propranolol 2 mg ⁄ kg ⁄ day is a useful treatment for severe or complicated IHs, achieving a rapid and significant reduction in their size.
This reduction was mainly achieved during the first 20 weeks of treatment, and further treatment induced a less dramatic therapeutic effect.
We did not include any patient with PHACE syndrome in our series, because we were concerned about potential effects of propranolol on congenital heart disease, aortic coarctation , or cerebral blood flow in patients with cerebral vascular disease.
This study had the limitation of being a retrospective open study, with no control group; furthermore, variable data collection of adverse events is also a limitation.
. A direct comparison with other modalities, mainly oral corticosteroids, was not carried out, and thus we cannot draw any conclusion about the compared efficacy of both treatments.
However, based on the authors’experience, we feel that propranolol’s therapeutic effects are at least as fast as corticosteroids.
Furthermore, we feel that propranolol is effective in situations where corticosteroids often fail, such as parotid region IHs and IHs located in the maxillary segment.
The duration of propranolol therapy is not well established, and the possible regrowth of IHs after propranolol withdrawal needs also to be addressed in long-term studies.
Propranolol is contraindicated in patients with asthma and it is recommended not to be used during episodes of bronchiolitis.
Very few adverse effects were observed in our series, and the ones that occurred were mild and did not imply dose reduction or treatment withdrawal.
Nightmares or agitated dreams were detected in 10 (14.1%) of 71 patients.
This is a known effect of propranolol, which usually does not require drug withdrawal.
None of our patients had symptoms of hypoglycemia, None of our patients had diastolic blood pressures below 40 mm that might have led to dose reduction.
We advise that a complete cardiologic study including physical examination and EKG should be performed before starting therapy.
In children with conflicting results or at high risk, echocardiogram is also advisable.
Monitoring blood pressure and heart rate during the first days of treatment is also recommended
In conclusion, in the series of patients in this observational study, oral propranolol 2 mg ⁄ kg ⁄ day was a well-tolerated and effective treatment for IHs.
More studies are needed to establish the optimal dose of propranolol and the appropriate duration of this treatment, as well as the comparative efficacy of propranolol with corticosteroids.

Response of a large IH to propranolol therapy: before treatment (A); at 4 weeks (B); at 8 weeks (C);and at 24 weeks (D).