Seminars in Cutaneous med surg 2011 – Elsevier
Chronic Pruritus – Pathogenesis, clinical aspects and treatment
Journal of the European Academy and venereology 2010
Key points
• Chronic pruritus is a common problem affecting a large proportion of the population.
• The pathophysiological mechanisms underlying chronic pruritus are still insufficiently understood .
• In the skin, diverse and complex interactions of keratinocyte, mast cells and sensory nerves largely determine the occurance and the control of pruritus.
• Systemic treatment with antihistamines often requires up-dosing to 4-fold of the recommended daily dose.
• Alternative systemic treatments of chronic pruritus are anticonvulsant drugs, µ-opioid receptor antagonists, antidepressants and UV light therapy.
• Novel treatment options for chronic pruritus are to be expected in the near future and include H4 receptor antagonists, К-opioid receptor agonists and neurokinin 1- receptor antagonists.
Introduction
Pruritus (itch) is a major symptom in many dermatologic as well as systemic diseases and has a dramatic impact on the quality of life in these patients.
The symptom of itch has to be treated on the basis of its pathophysiology and its underlying disease.
In daily practice, a“quick” diagnosis of the underlying disease is often difficult, although a rapid relief of the itch is desired.
We often treat patients on the basis of the symptomatology.
A rational therapeutic ladder for a symptomatic therapy is useful until the final diagnosis has been confirmed.
There are probably many subtypes of pruritus, just as there are many diseases that cause itch. The pathophysiology in many subtypes of pruritus is still poorly understood,
hindering a rapid and targeted treatment strategy.
An extensive diagnostic workup is often
required to determine the final cause(s) of the itch. Thus, in daily life, physicians often start with a more or less rational therapeutic strategy to combat the debilitating itch.
On the basis of our current knowledge about the different pathophysiologies of itch, on clinical trials or case reports, and our own clinical experience, we aim to present therapeutic ladders for the rapid as well as long-term management of itch.
Classification of itch
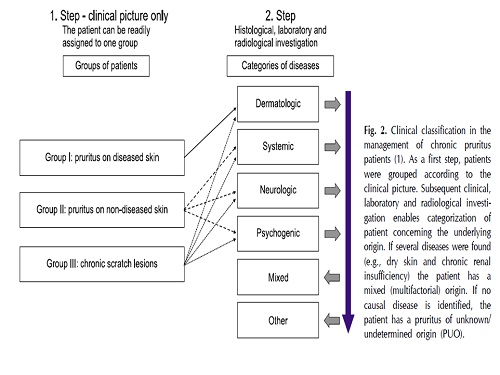
Pathophysiology of itch
In the skin,many factors contribute to the induction,exacerbation or suppression of pruritus.
Physical stimuli : painful heat and cold
Mechanical factors : rubbing or scraching
Resident skin cells : keratinocytes –
mast cells (have a central role in the cellular network of pruritus.it can induce pruritus via H1 receptors on nerve fibres. Apart from H1 receptors, histamin modulates pruritus also by H3 and H4 receptors. While the pharmacological blockade of H4 receptors has been shown to reduce pruritus significantly in mouth models,H3 receptors appear to be involved in the suppression of pruritus as H3 receptor antagonists have been shown to induce pruritus in mice.
Pure histamine –induced itch is rare.This is reflected in the excellent antipruritic effect of antihistamines in urticaria and their limited effect in other itch- associated disorders).
Infiltrating cell : eosinophils (that can contribute to the enhanced levels of nerve growth factor measured in the skin of AD patients and thus to the persistence of pruritus in these patients.
T- cell derived interleukin-31( has recently been shown to induce severe pruritus in mouse models of AD and to be highly up-regulated in the skin of AD patients.
NEUROPEPTIDES
Several observations support the idea of an important role
of neuropeptides for the pathophysiology of pruritus in
various skin diseases.
Neuropeptides such as SP, vasoactive intestinal peptide (VIP), somatostatin, and neurotensin provoke itch along with the characteristics of neurogenic inflammation such as erythema, wheal and flare.
SP induces itch responses in human and mice which are mediated via activation of the neurokinin 1 receptor (NK1R) on mast cells and keratinocytes resulting in
enhancement of inflammatory responses supporting a indirect effect of SP in mediating pruritus.
Targeting the neuropeptides is a new concept in the treatment of itch. For example, a case series applying the NRK1 antagonstis
aprepitant showed significant antipruritic effects in patients
with prurigo nodularis and atopic predisposition Controlled trials are pending.
Therapy of Pruritus
• Elimination of triggering factors
• Topical antipruritic therapies
• Systemic Therapies:
• Antihistamines/Mast Cell Stabilize
• Systemic Glucocorticosteroids
• Other Immunosuppressants
• Thalidomide
• Opioid-Receptor Antagonists and Agonists
• Antipruritc Antidepressants
• Antipruritic Anticonvulsants
• Phototherapies
• Novel and Experimental Therapies
Elimination of triggering factors
• Physical factors:overheated rooms, insulating clothing, being in a warm bed.Also,factors that irritate the surface of the skin:rough fabrics or wool clothing should be avoided.
• Dry skin: before doing anything else,a moisturizing therapy should be initiated as a basic therapy.
• Internal factors: hot spices,alcohol,hot beverages, medications(ß-blockers, allopurinol)
• Psychogenic factors: tension and stress
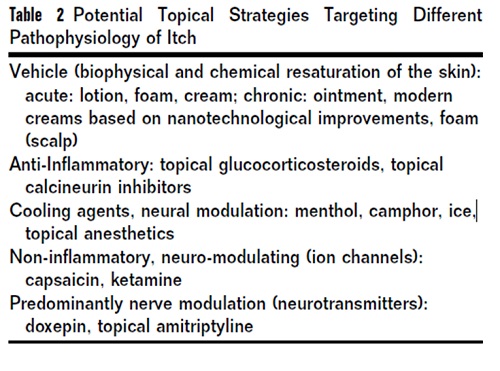
Topical Therapies
Although not completely effective in most of the cases, topi-therapy is an important part of a successful therapeutic intervention. Here, the best vehicle must be chosen (lotion or cream for acute phase, ointment for chronic phase and xerosis).
alternatively, modern creams such as Cetaphil RESTORADERM(Galderma Canada Inc, Thornhill ON, Canada), which have moisturizing epidermal properties of the epidermis, can be used for both acute and chronic pruritus.
In the past few years, there have been reports on the use of topical canabinoid agonists for treatment of pruritus in experimentally induced pruritus as well as in patients with atopic dermatitis.
Systemic Therapies�
Although various systemic therapies have been used to treat pruritus, no randomized controlled trials have shown one
medication to be the most effective and safe. Most studies are case reports, case series, or open trials without long-term follow-up.
Although recent basic research revealed the existence of certain histamine-independent itch pathways, no unique itch biomarker or therapy is on the horizon for all subforms of pruritus.
Here, we focus on treatments that can be used by patients seen in daily practice who have moderate to severe chronic pruritus. In these cases, a therapeutic ladder is a promising approach to control pruritus.
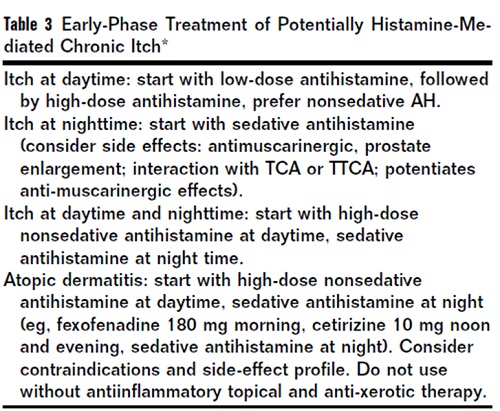
Antihistamines/Mast Cell Stabilizers
Recent studies indicate a role of H1R and H4R in certain subforms of itch. So far, only H1R antagonists are available for treating pruritus and allergic diseases.
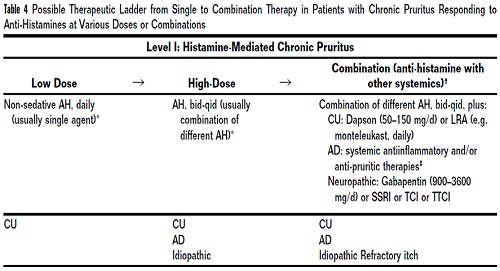
Nonsedative H1R antagonists are recommended in most forms of urticaria.
Often greater doses (three to four times greater than recommended antiallergic doses) become effective as an antipruritic regimen.
If low-dose as well as high-dose antihistamines fail, non-antihistamines agents are necessary.
In general,high-dose antihistamine (AH) regimens are well tolerated.
Side effects (antimuscarinergic effects, sedation, antimotion effects) and contraindications have to be considered, especially in elderly patients, because of potential arrythmias or renal dysfunction attributable to some AH.
Except for urticaria, the efficacy of systemic AH in pruritic diseases has been poorly documented in randomized,double-blind, placebo-controlled clinical trials.
Doxepin 10-100 mg d1 has been a widely used strategy to combat various subforms of pruritus.
It has antihistaminergic, antiserotoninergic, and antiadrenergic effects and is a relatively safe drug with a long history of use.
Gradual dose escalation (e. g., starting at 10 mg and adding 10 mg every third night) is important.
In 19 clinical trials between 1950 and 2009, topical doxepin was the only AH that showed efficacy for the treatment of chronic pruritus.
Thus, topical doxepin may be an alternative to systemic treatment with less sedation.
doxepin not infrequently causes allergic contact dermatitis.
In general, we prefer an “add-on” approach instead of a replacement strategy.
a nonsedative AH in the morning (eg, fexofenadine or loratadine), a nonsedative or mildly sedative AH in the afternoon (e. g., azelastine, cetirizine), and a mildly sedative or sedative AH in the evening/at night (first generation AH), if there are no contraindications (e. g., renal disease, age, risk of arrhythmia).
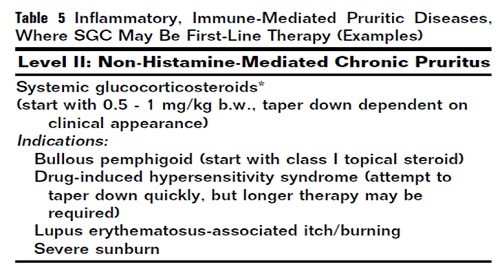
systemic Glucocorticosteroids
SGCs decrease edema, leukocyte migration and phagocytosis and are effective in many pruritic diseases, such as AD, psoriasis,urticaria, lupus erythematoses, bullous pemphigoid,lichen planus, cutaneous T-cell lymphoma, and some causes of drug.
The kinetics of the antipruritic effect of SGCs matches the antiinflammatory action of SGC, indicating that cytokines(e. g., interleukin [IL]-6, IL-31), chemokines, and lipid mediators(e. g., PGE2) may be also involved in pruritus.-induced pruritus.
The use of SGC should be limited to controlling acute,severe forms of pruritus.
For patients with AD, SGCs are not necessary.
Note that AD is not included, and that in many diseases SGC are even not second- or third-line therapy.
In many instances of mentioned first-line indications, class 1 topical GCs have been demonstrated same efficacy with less side effects.
Immunosuppressants
Cyclosporine A has been shown to be effective for the treatment of itch in AD and certain autoimmune diseases.
Successful treatment of prurigo nodularis of different origin has been described in 16 patients with an efficacy of 92% and a side effect profile of 50%.
Cyclosporine A may be also effective in other pruritic diseases that have a dominant T cell infiltrate, like lichen planus or drug-induced pruritus.
Adjusted for renal function, cyclosporine A can be started at 3-5 mg/kg body weight, and later reduced to 3 mg/kg.
The benefit of other systemic immunosuppressants, such ascyclophosphamide, tacrolimus, mycophenolate mofetil, and azathioprine, as antipruritic agents is poorly documented.
Thalidomide
Thalidomide is used in doses between 25 and 400 mg/d in pruritic diseases.
A beneficial effect of thalidomide (200 mg/d) was reported in a patient with severe pruritic Hodgkin lymphoma.
Successful therapy of prurigo nodularis has also been described at a low dose of 100 mg/d or less.
Opioid-Receptor Antagonists and Agonists
Opioids are important transmitters in the pain pathways opioid receptors (mu, kappa, delta)
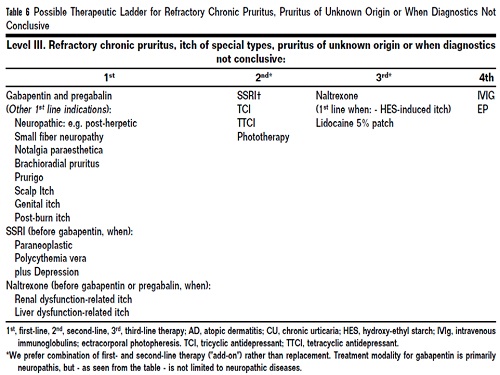
Although activation of mu-opioid receptors results in pruritus activation of kappa opioid receptors suppresses itch at the spinal cord. the efficacy of mu-opioid receptor antagonists like naloxone (intravenously) or naltrexone (orally) is well documented in randomized and other controlled clinical trials.
Because of its side effects, including drowsiness, dizziness,sedation, and gastrointestinal disturbances, the dose of naltrexone should be gradually increased (starting at 25mg, adding 25 mg every third day until 100 mg).
The kappaopioid receptor agonist TRK-820 (nalfurafine) is approved for the treatment of renal itch.
Current trials are investigating the effectiveness of nalfurafine in atopic dermatitis.
Antipruritc Antidepressants
SSRIs have been used to treat pruritus in patients with:
prurigo
AD
psychogenic pruritus
paraneoplastic pruritus
polycythemia vera
Effectiveness has been documented with paroxetine, 20 mg/d, fluvoxamine, and sertraline.
Sertraline, 75-100 mg/ d has been successfully used in cholestatic pruritus.
A combination of sertraline and gabapentin was successfully used in patients with cutaneous Tcell lymphoma (CTCL).
Antipruritc Antidepressants
Doxepin(10-100 mg oral) acts on serotonin-, histamine-, and noradrenergic receptors. In our experience, low-dose
doxepin is also useful in patients with:
renal itch
atopic dermatitis
various pruritic non-inflammatory dermatoses
HIV-induced pruritus
Unfortunately, its effectiveness is rather unpredictable.
Patients start with 10 mg of doxepin at night,which is up-dosed every third day until the level of sedation is no longer tolerable.
Because of their sedative and antimuscarinergic effects, TCAs should be considered as second or third-line therapy.
No large controlled studies have compared the effects of TCAs, tetracyclic antidepressants (TTCAs), SSRIs or SNRIs with respect to efficacy, safety and tolerability
Mirtazepine mainly acts as a serotonin- and dopamine-reuptake inhibitor.
We find mirtazepine at doses between 15 and 30mg/d beneficial for chronic pruritus of different causes.
Mirtazepine is helpful as a prophylaxis of morphine-induced pruritus
some patients complain that in addition to the effects of TCA they experience weight gain and generalized edema.
Anticonvulsants that have been tested for their ability to suppress itch are gabapentin and its prodrug, pregabalin.
their ability to modulate calcium channels, inhibit glutamate synthesis and release, and/or inhibit GABA-ergic pathways in the central nervous system.
brachioradial pruritus
Notalgia Paresthetica
senile pruritus
postburn itch
morphine-induced Itch
CTCL
liver-associated
renal itch
Dosages vary between 900 and 3600 mg of gabapentin daily .
The side effect profile of gabapentin Includes: back pain, blurred vision, constipation, diarrhea,drowsiness, dry mouth, nausea, stomach upset, tiredness, vomiting, and weight gain.
Contraindications are allergies and risk of seizures.
Phototherapies
Effective in pruritus of different aetiologies.
Especially useful in patients with:
Contraindications to systemic agents
During late-term pregnancy
In older patients
In those with multiple prior disease or who are taking several medications
In patients who other antipruritic therapies have failed
Its immunomodulatory effects make phototherapy especially useful for treating inflammatory dermatoses.These effects are mainly caused by the inhibition of proinflammatory mediators, such as IL-1 and tumor necrosis factor-lapha, or release of anti-inflammatory neuropeptides.
UV radiation exerts an immunosuppressive and anti-inflammatory effect in various pruritic inflammatory skin diseases,including AD, or by modulating proliferation and apoptosis in neoplasms like CTCL.
A direct impact of UV light on sensory nerves during neoplastic processes is still underdebate. Thus, whether UV radiation may have a direct beneficial effect on sensory nerves by controlling neuronal function is not known.
inflammatory dermatoses
CTCL
solar urticaria (hardening)
systemic diseases (cancer-associated itch, renal itch, liver-associated itch(
atopic dermatitis
Prurigo nodularis
Solar urticaria
aquagenic pruritus
CTCL
Hodgkin lymphoma
polycythemia vera
HIV infection
folliculitis of pregnancy
UV light therapy is not advised for patients who are taking topical calcineurin inhibitors.
Novel and Experimental Therapies
In recent years,pruritus has gained more and more attention and is appreciated as an important symptom that can dramatically reduce quality of life in patients. This new focus on itch as a specific target has lead to the development of novel drugs that are currently tested in clinically trials or which are currrently under development. Among them are for example histamine H4 receptor antagonist and κ-opioid agonists.
Furthermore some drugs have been reported in case reports or small case series to be highly effective in suprissing pruritus. For example, the neurokinin -1 receptor antagonist aprepitant was shown to be able to control almost completely the severe and treatment refractory pruritus in three patients with sezary syndrome and 20 patients with pruritus and prurigo nodularis. Randomized controlled trials have to be performed to test the potential of this substances to be used as novel antipruritic drugs.

